Hypokalemia, a condition characterized by abnormally low levels of potassium in the blood, can have significant implications for cardiac health. One of the critical diagnostic tools used to assess the encroachment of hypokalemia on the heart is the electrocardiogram (ECG). Understanding the relationship between ECG in hypokalemia is essential for healthcare professionals to accurately diagnose and manage this stipulation.
Understanding Hypokalemia
Hypokalemia occurs when the potassium level in the blood falls below 3. 5 mmol L. Potassium is all-important for maintaining normal heart purpose, muscle and nerve action, and overall cellular health. Low potassium levels can take to various symptoms, including muscle weakness, fatigue, and in severe cases, life threatening cardiac arrhythmias.
Role of ECG in Diagnosing Hypokalemia
The ECG is a non invasive test that records the electric action of the heart. It is a valuable tool for detecting abnormalities in heart rhythm and conduction that may be connect with hypokalemia. The characteristic changes in the ECG due to hypokalemia include:
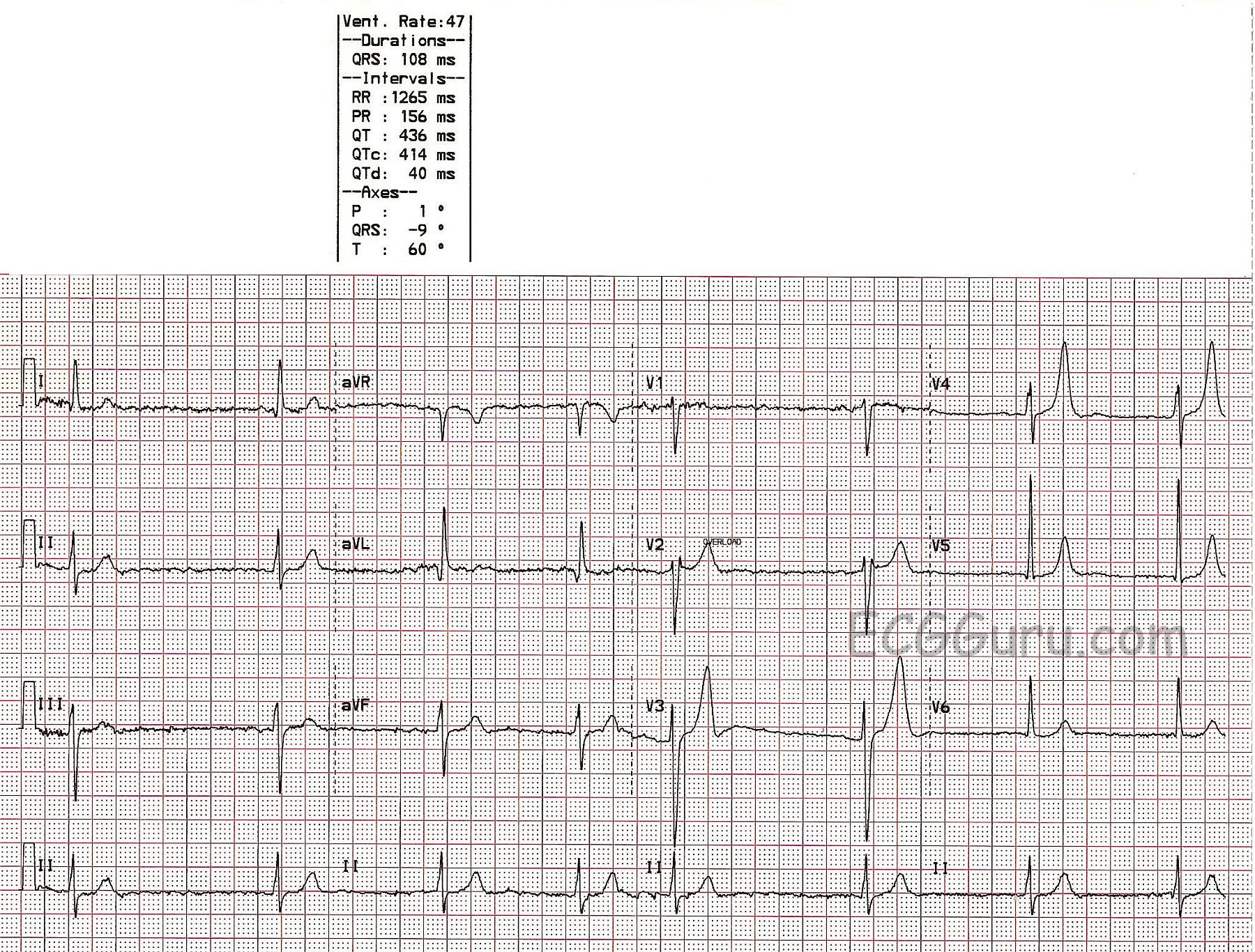
- T wave flatten or inversion: This is one of the earliest signs of hypokalemia on an ECG. The T waves, which represent the repolarization of the ventricles, turn flatten or invert.
- ST segment slump: The segment between the end of the QRS complex and the commence of the T wave may be depressed, indicating unnatural repolarization.
- U waves: Prominent U waves, which are modest deflections postdate the T wave, can be seen in hypokalemia. These waves are normally not visible but turn outstanding when potassium levels are low.
- Prolonged QT interval: The QT interval, which represents the time from the start of the Q wave to the end of the T wave, may be prolonged. This can increase the risk of ventricular arrhythmias.
- Arrhythmias: Severe hypokalemia can conduct to several arrhythmias, include atrial fibrillation, ventricular tachycardia, and ventricular fibrillation.
Interpreting ECG Changes in Hypokalemia
Interpreting ECG changes in the context of hypokalemia requires a taxonomic approach. Here are the steps to accurately interpret an ECG in a patient with mistrust hypokalemia:
- Assess the T waves: Look for flatten or inversion of the T waves, especially in the precordial leads (V2 V6).
- Evaluate the ST segment: Check for slump of the ST segment, which can be subtle and may require heedful measurement.
- Identify U waves: Look for spectacular U waves following the T waves. These waves are best seen in the precordial leads.
- Measure the QT interval: Calculate the QT interval and correct it for heart rate using the Bazett's formula (QTc QT RR). A sustain QTc interval may point an increase risk of arrhythmias.
- Check for arrhythmias: Look for any signs of atrial or ventricular arrhythmias, which can be life menace in severe hypokalemia.
Note: It is important to correlate ECG findings with serum potassium levels and clinical symptoms to confirm the diagnosis of hypokalemia.
Management of Hypokalemia
Once hypokalemia is diagnose, prompt and seize management is important to prevent complications. The management strategies include:
- Potassium subjunction: Oral potassium supplements are typically the first line of treatment for mild to curb hypokalemia. Severe cases may require endovenous potassium replacement under close monitoring.
- Identify and treat the underlying induce: Hypokalemia can be do by various factors, including diuretic use, gi losses, and endocrine disorders. Treating the underlying get is indispensable to prevent recurrence.
- Monitor ECG and electrolytes: Regular monitoring of ECG and serum potassium levels is necessary to assess the response to treatment and prevent complications.
- Avoid triggers: Patients should avoid factors that can worsen hypokalemia, such as excessive use of diuretics, laxatives, or licorice.
Case Studies and Examples
To illustrate the importance of ECG in hypokalemia, let's consider a few case studies:
Case Study 1: Mild Hypokalemia
A 45 year old patient presents with muscle weakness and fatigue. The ECG shows flatten T waves and mild ST segment slump. Serum potassium point is 3. 0 mmol L. The patient is part on oral potassium supplements, and the symptoms resolve within a few days. Follow up ECG shows normalization of T waves and ST segment.
Case Study 2: Severe Hypokalemia
A 60 year old patient with a history of diuretic use presents with palpitations and dizziness. The ECG shows large U waves, T wave inversion, and a prolonged QT interval. Serum potassium level is 2. 5 mmol L. The patient is admitted to the hospital for intravenous potassium replacement and cardiac monitor. The arrhythmias resolve, and the ECG normalizes with treatment.
Case Study 3: Hypokalemia with Arrhythmias
A 70 year old patient with a history of chronic kidney disease presents with syncope. The ECG shows atrial fibrillation with a rapid ventricular response and large U waves. Serum potassium stage is 2. 8 mmol L. The patient is steady with endovenous potassium and antiarrhythmic medications. The arrhythmia converts to sinus rhythm, and the ECG normalizes with treatment.
Preventing Hypokalemia
Preventing hypokalemia involves name and cope risk factors. Some preventive measures include:
- Adequate potassium intake: Ensure a equilibrate diet rich in potassium, including fruits, vegetables, and whole grains.
- Monitor diuretic use: Regularly admonisher potassium levels in patients taking diuretics and adjust the dosage as needed.
- Avoid excessive laxative use: Limit the use of laxatives, which can cause gastrointestinal losses of potassium.
- Manage underlying conditions: Properly handle conditions that can lead to hypokalemia, such as diabetes, hyperaldosteronism, and gi disorders.
Note: Regular supervise of serum potassium levels and ECG in eminent risk patients can facilitate detect and deal hypokalemia early.
Conclusion
Hypokalemia is a mutual electrolyte upset that can have substantial cardiac manifestations. The ECG plays a crucial role in name and grapple hypokalemia by detecting characteristic changes in the electrical action of the heart. Prompt acknowledgment and treatment of hypokalemia are essential to prevent life imperil arrhythmias and other complications. Healthcare professionals should be vigilant in supervise serum potassium levels and ECG in patients at risk for hypokalemia to ensure apropos interference and optimal outcomes.
Related Terms:
- ecg changes with hypokalaemia
- u waves in hypokalemia
- drugs causing hypokalaemia
- ecg signs of hypokalemia
- hypokalemia ecg changes mnemotechnical
- drugs that get hypokalemia